Part 1: What the Glucosamine Bioavailability Research Actually Shows for Senior Dogs
This is part 1 of a four-part series on senior dog joint supplements. Click to see my full senior dog joint supplement series.
This is a research summary, not veterinary advice. I’m a science writer and biologist, not a clinician. For your dog specifically, work with your vet.
Understanding Glucosamine Bioavailability in Dogs
My dog Butters
My oldest dog, Butters, is nine years old (as of 2026). She is, by most measures, still doing well and can still jump up on my bed, jump into the Wisconsin River when hunting for sticks, and jump into my car, without assistance or worry. At night, she sleeps the kind of sound, full sleep that older dogs sleep when they’ve had a real day. But Butters isn’t the young pup that I adopted back in 2018. I’ve grown concerned about her overall health after seeing her limping during an extended session of stick fetching on the water. She sometimes also limps after jumping on, and then off, my bed. Sadly, osteoarthritis may be creeping up on her.

I started looking at joint supplements shelf at some of my local pet supply store and found myself overwhelmed by the myriad of choices. There was the standard glucosamine and chondroitin, but there were others too, like MSM, turmeric, and even green-lipped mussel. The supplements weren’t cheap either: typical tablets that you need to break apart into food run about 50-cents/day, and the tastier one-a-day chews cost roughly $60/month. Every single bottle or box of supplement makes confident claims about its effects on hip and joint health- but can these claims be verified?
Before spending money on different supplements and hoping one of them worked on Butters, I stopped and read the actual research.
What I learned was not what I expected. Of course, the pet supplement industry tells you that these compounds work. The cynical side of the online world tells you that joint supplements are nothing more than snake oil. The truth, which is harder to fit on a bottle, is that the research ‘proof’ is mixed. Also, almost no research publication answers the question you’re really hoping to answer: Will the supplement you just bought actually reach the joint you’re trying to help?
That question, by the way, is called bioavailability.
Bioavailability is what this blog post is going to delve into, explain, and try to figure out from what the canine research data show.
Dog joint supplements are big business
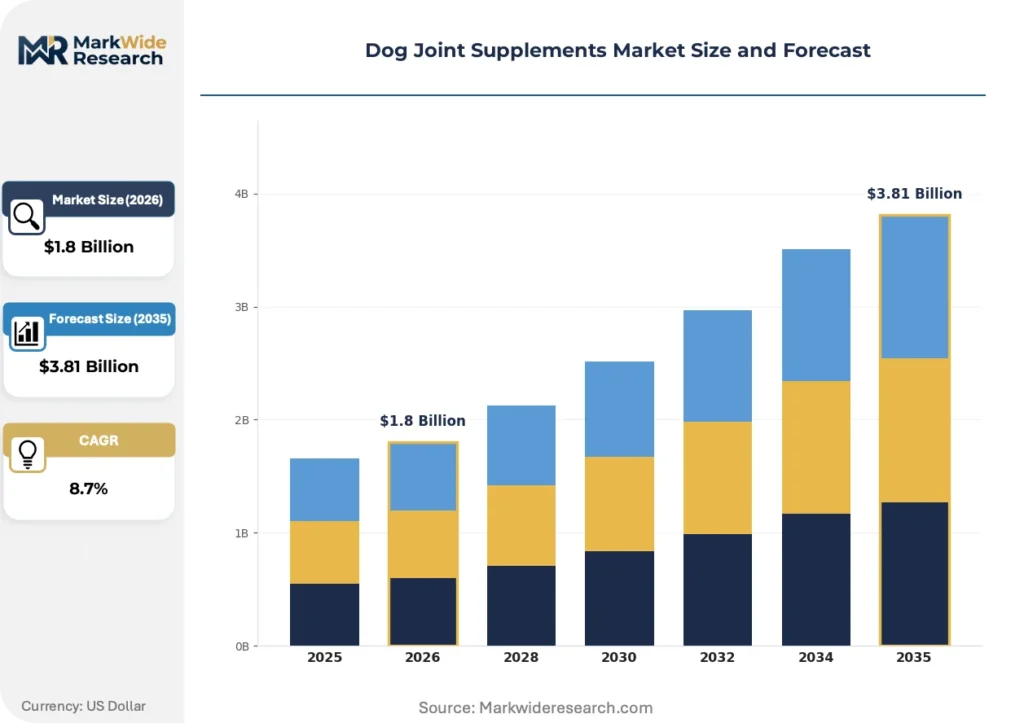
Glucosamine-chondroitin supplementation for senior dogs is one of the most common interventions in pet care. Pet supply stores, vet clinics, online sites like Chewy- offer dozens of variations of the same basic product: a tablet or soft chew containing some combination of glucosamine and chondroitin sulfate, along with possible MSM, omega-3, or even the new-fangled mussel extract. Little wonder: The senior pet supplement market (in the USA) is growing, and and joint health supplements represent a significant share of it. Just check out this graphic below, which provides a forecasted compound annual growth rate, or CAGR, of 8.2% for dog joint supplements and is derived from data published by MarketWide Research:
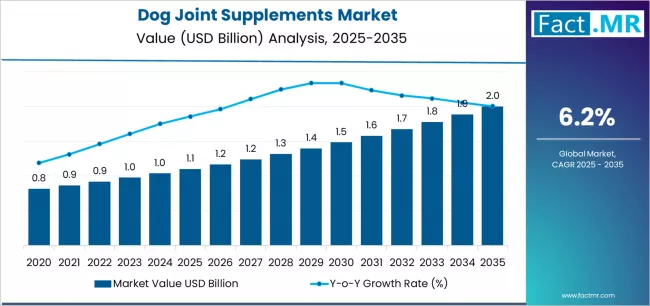
This report, compiled by Fact.MR, gives a forecasted CAGR of 6.2% for dog joint supplements, predicting it to go from the current $1 billion figure in 2025 to $2 billion by 2035:
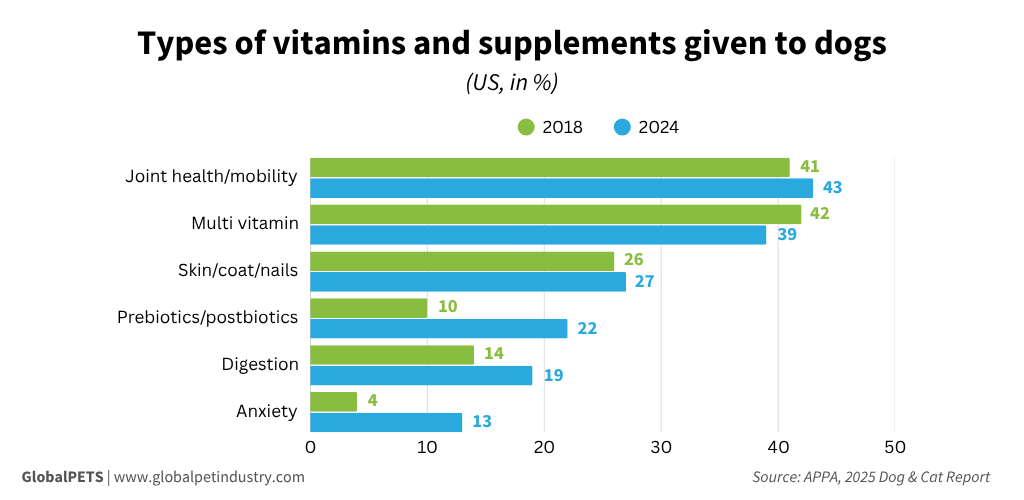
These data, compiled by the American Pet Products Association and published in 2025, showcase joint supplements as the leading supplement being given to dogs.
There are several reasons for this trend:
- Veterinarian recommendations. Many vets recommend glucosamine-chondroitin supplements as a ‘why not?’ treatment for senior dog with early arthritis or mobility concerns. There are few or no serious side effects in most dogs, and the cost is manageable. Compared to NSAIDs, which are more effective but carry real risks of gastrointestinal, renal, and hepatic side effects, supplements feel like a gentler first step. Many vets recommend starting supplements before any clinical signs appear, with the theory being that they may slow cartilage degradation if started early enough.
- Aggressive marketing. You can’t help but be bombarded with joint supplement marketing anywhere you look. In vet clinics, the strategically placed brochures and product labels do well to make their claims seem legit: of course, products A, B, and even F are vet-recommended. Pet stores have entire aisles dedicated to supplements, making it seem like every dog owner is giving their dog a compound “boost” of some kind. The marketing has a one-going-on-two-billion-dollar reason behind it:
- Emotional strings that pull. One big side effect of all this supplement marketing is emotional. You feel guilty that you aren’t concerned enough about your aging dog’s joints and risk of developing OA. When you see your dog struggle to get up, or limp for no reason, you want to do something to help them out. Supplements become that natural first choice, and especially because they’re available without prescription.
As a result, many senior dogs are on some version of glucosamine-chondroitin at some point in their lives. However, whether the supplements are actually doing what they claim…. well, that’s a different matter entirely- and it’s what this article is all about.
Dose ≠ Bioavailability ≠ Efficacy
The number on the label doesn’t tell you what your dog actually absorbs — or if it even works.
Whether a joint supplement “works” feels like one question, but it’s actually two questions stacked on top of each other.
The first question is whether the active molecule, when given orally, reaches the joint in meaningful amounts. This is the crux of bioavailability. A supplement can contain whatever dose the manufacturer prints on the label, but the dose on the label is not the dose that reaches your dog’s cartilage. The journey from chew to joint involves dissolution in the stomach, absorption across the gut wall, passage through the liver (where some compounds are metabolized before reaching the rest of the body), distribution through the bloodstream, and finally, crossing from blood into the joint tissue itself. At each step, some of the original dose is lost. The question of bioavailability is, in essence, how much actually arrives where it’s supposed to act?
The second question is, at whatever concentration the supplement does reach the joint, does it actually do anything biologically useful? This is what I mean by efficacy. Even if a compound has well-established effects in laboratory studies on cartilage cells growing in a Petri dish, that doesn’t mean that dosing a live arthritic dog with the same compound will improve its mobility, pain, or quality of life.
These questions are often glossed over in marketing, because the objective is to make the (recurring) sale. Also, the answer to one of these questions doesn’t necessarily determine the answer to the other.
This blog post is about the first question: bioavailability. In part 2 of this blog series, I’ll address efficacy.
What are Glucosamine and Chondroitin?
Before going further, let’s explore what these two compounds are at the molecular level.
Glucosamine is an amino sugar, consisting of a glucose-like sugar ring with an amine group attached. The body uses it as a building block for glycosaminoglycans, or GAGs, which are long chains of sugar-derived molecules that form a major component of cartilage. Cartilage is the smooth tissue that cushions the ends of bones inside joints, and GAGs are what give cartilage its ability to hold water, absorb shock, and resist compression. When cartilage degrades (a major cause of OA), the GAG matrix breaks down, and the joint loses its cushioning.
The theory behind glucosamine supplementation is that providing extra glucosamine in the diet gives the body raw material for GAG synthesis, which might support cartilage maintenance and/or repair. Whether this is reality or merely a nice theory is being tested continuously.
Glucosamine appears in supplements in two different formulations. Glucosamine hydrochloride (HCl) is mostly intended for use in dogs, while glucosamine sulfate is intended for human use and has been studied more extensively in human OA. The two forms deliver the same active molecule but differ in their associated salt, which affects how the compound behaves in the stomach and bloodstream. Whether one form is more bioavailable than the other in dogs has limited research backing. It comes up frequently enough in marketing claims, though, so we’ll return to this topic later.
Chondroitin sulfate is a larger and more complex molecule. While glucosamine is a small sugar, chondroitin sulfate is a long polysaccharide with attached sulfate groups. Chemically speaking, it is a sulfated glycosaminoglycan (GAG) composed of a long chain of alternating sugars (N-acetylgalactosamine and glucuronic acid). Physiologically, chondroitin sulfate is actually “built” by glucosamine and is a major structural component of cartilage. Without it, much of the compressive strength and water-retention capability of cartilage would not exist.
Because chondroitin is so big, it’s not absorbed in its starting form in the blood. In other words, most chondroitin doesn’t reach the bloodstream as intact long-chain molecules; it’s actually broken down into smaller disaccharide units in the gut and reassembled later. On a side note, the pharmacokinetic papers that report chondroitin levels post-dosing are actually reporting its disaccharide levels.
Glucosamine and chondroitin are often sold together because they’re hypothesized to work synergistically, with glucosamine acting as the building blocks, and chondroitin acting as the scaffold that those glucosamine building blocks attach to. Here are both of the molecules, shown side-by-side:
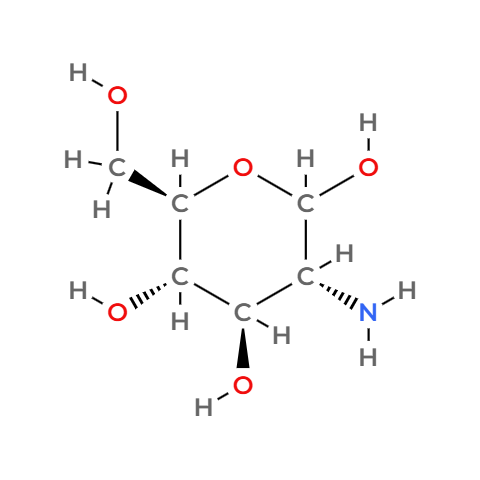
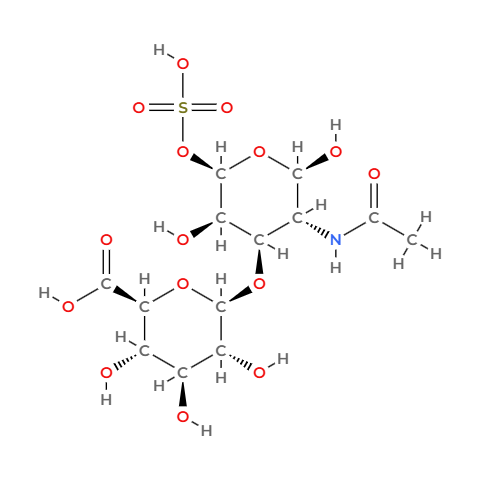
Glucosamine and chondroitin sulfate. Left: glucosamine’s 2D skeletal structure, showing the six-membered sugar ring with an amino group (NH) attached to the second carbon. This amino group makes it an “amino sugar” rather than just plain glucose. Right: a single disaccharide unit of chondroitin sulfate, showing the sulfate group (SO₃) and acetyl (COCH₃) groups that are characteristic of the compound. In the body, chondroitin sulfate exists as a long polysaccharide chain made of hundreds of these repeating units. Structures were rendered in MolView.
What is bioavailability?
Bioavailability is one of those words that scientists, especially pharmacologists, use precisely …and marketers use in any way that makes them a sale. Speaking precisely, the definition of bioavailability is: the fraction of an administered dose that reaches the systemic circulation in unchanged form. In this case, “systemic circulation” means the bloodstream.
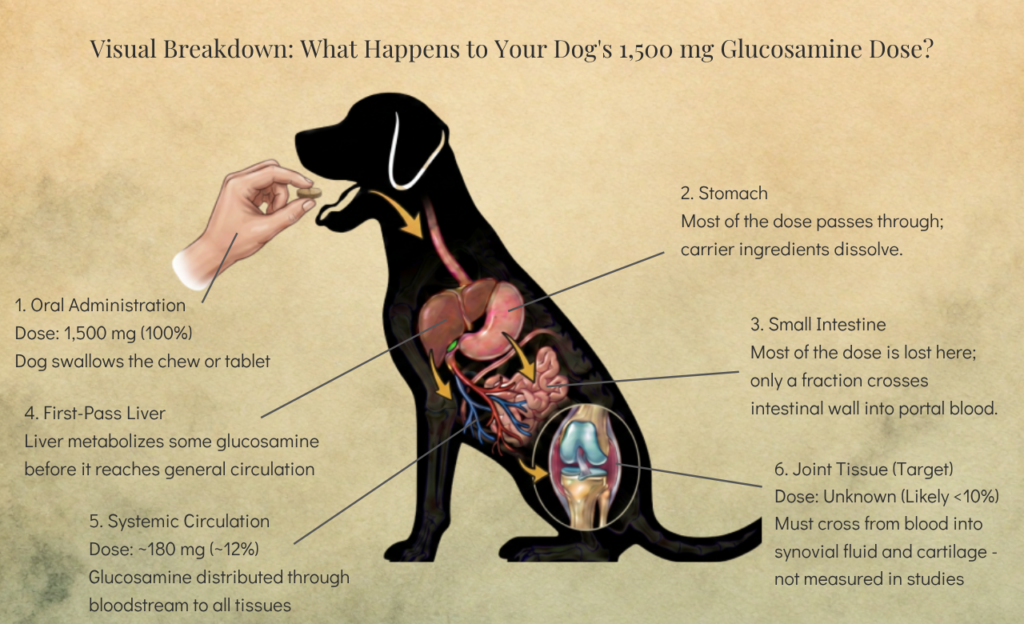
The reason this matters is that nothing you swallow gets to its target intact. A 1,500 mg dose of glucosamine doesn’t deliver 1,500 mg of glucosamine to the bloodstream. It delivers some fraction of that, and the rest is lost along the way via biological filters and barriers.
The journey looks roughly like this. The chew or tablet enters the stomach, where it must first dissolve. Stomach acid begins to break down the carrier ingredients and release the active molecules. The released compound then passes into the small intestine, where it must cross the intestinal epithelium — the thin layer of cells that separates the gut lumen from the bloodstream. Some compounds cross easily; others, depending on size, charge, and chemical stoichiometry, cross slowly or not at all. Whatever does cross enters the portal vein, which carries blood directly to the liver. The liver is the body’s primary detoxification organ, and it metabolizes many ingested compounds before they reach the bloodstream. This is called the first-pass effect. For some drugs, it dramatically reduces the dose that ultimately reaches the rest of the body. Whatever survives the first pass enters systemic circulation, where it can be distributed to tissues and, theoretically, joints.
So, going back to glucosamine, while the label on the bottle says it contains 1,500 mg of glucosamine per dose, the entire 1,500 mg is ultimately not reaching the joint. If, for example, only 10% of the dose actually crosses the gut wall, survives the liver, reaches the bloodstream, and is then delivered to the joint cartilage, then the biologically meaningful dose is 150 mg, which is an order of magnitude less than advertised.
This is why bioavailability has to be the first question. Without knowing whether the effector molecule even reaches the target tissue in meaningful amounts, there can be no discussion of clinical effects.
What the canine research shows
The foundational study on glucosamine bioavailability in dogs was published in 2002 by Abimbola Adebowale and colleagues at the University of Maryland School of Pharmacy, in the journal Biopharmaceutics and Drug Disposition. It is, more than two decades later, still the most-cited pharmacokinetic study on oral glucosamine in dogs, and most reviews of canine joint supplements trace back to this paper.
The study used eight male beagle dogs, each weighing approximately 12 kilos (or 26.5 lbs). The product that was tested was Cosamin/Cosequin, a supplement manufactured by Nutramax Laboratories that combines glucosamine hydrochloride with low-molecular-weight (LMW) chondroitin sulfate. Incidentally, the study was also funded by Nutramax (a point I’ll address later).
The researchers used four treatment protocols across the same group of dogs. The first treatment was intravenous administration of glucosamine (500 mg) and chondroitin sulfate (400 mg). The IV route delivers 100 percent of the dose to systemic circulation by definition, bypassing the gut and the liver entirely. Comparing IV plasma concentrations to oral plasma concentrations is how oral bioavailability is calculated, with the IV route being the reference for what “complete absorption” looks like, and the oral route measured against it.
The second and third treatments were single oral doses at two different levels: glucosamine 1,500 mg with chondroitin 1,200 mg, and glucosamine 2,000 mg with chondroitin 1,600 mg. The fourth treatment was actually a multi-dosing protocol which was intended to mimic actual daily supplementation, so the 1,500 mg of glucosamine and 1,200 mg of chondroitin were given once daily for seven days, then raised to 3,000 mg and 2,400 mg for the second week.
Blood samples were collected over 24 hours after each dose, and the researchers measured plasma concentrations of glucosamine and of chondroitin sulfate disaccharides.
For simplicity, here is the entire study design:
Adebowale et al. (2002) Study Protocol
| Parameter | Details |
| Study Population | 8 male beagle dogs, ~12 kg (~26.5 lbs) |
| Product Tested | Cosamin/Cosequin (Nutramax) — glucosamine HCl + LMW chondroitin sulfate |
| Treatment 1 (IV) | Glucosamine 500 mg / Chondroitin 400 mg (bioavailability reference) |
| Treatment 2 (Oral) | Glucosamine 1,500 mg / Chondroitin 1,200 mg (single dose) |
| Treatment 3 (Oral) | Glucosamine 2,000 mg / Chondroitin 1,600 mg (single dose) |
| Treatment 4 (Multi-dose) | Days 1-7: 1,500/1,200 mg QD; Days 8-14: 3,000/2,400 mg QD |
| Sample Collection | Blood samples over 24 hours post-dose |
| Measurements | Plasma concentrations of glucosamine and chondroitin disaccharides |
What they found was that, with glucosamine HCl, oral bioavailability was ~12%. This number has been cited by almost every subsequent review of canine joint supplement pharmacokinetics. After the 1,500 mg oral dose, the peak plasma concentration (Cmax) was 8.95 micrograms/milliliter (μg/mL), reached about 1.5 hours after dosing (Tmax). So, glucosamine was absorbed relatively quickly. After IV administration, glucosamine also cleared from the plasma quickly, with an elimination half-life of about 31 minutes. It doesn’t linger in the circulation very long.
With chondroitin sulfate, single-dose bioavailability was 4.8-5%. The chondroitin Cmax was 21.5 μg/mL after the 1,600 mg dose, with an area-under-the-curve (AUC) of 187 microgram-hours/mL. The most striking finding for chondroitin came with multiple dosing: after repeated daily administration, bioavailability rose to between 200-278%. This suggests chondroitin or its breakdown products accumulate in plasma with repeated dosing. It also means that single-dose measurements underestimate what happens during real-world supplementation.
So…while a 12% (of 1,500 mg, or 180 mg) glucosamine bioavailability report is significant, it may, or may not be, enough to produce the desired clinical effects that it’s touted for. But, at least the molecule in question gets to its final destination.
However, 12% is also not 100%. The gap between what the label says and what reaches the bloodstream is significant. A pet owner reading “1,500 mg glucosamine per serving” on a product label is implicitly being told that that’s the dose the dog receives; however, the label dose and the biologically active dose are not the same.
As for the chondroitin numbers, the systemic accumulation of this molecule is intriguing. It means that single-dose studies may underestimate chondroitin’s actual absorption, and the cumulative effect of daily dosing matters more than any single dose. Does this accumulation have clinical relevance for joint health? That’s a separate question.
There’s one more twist to the chondroitin story, and it’s a useful lesson in reading bioavailability numbers skeptically. Adebowale’s ~5% figure isn’t the only one in the literature. Back in 1995, a team led by Conte fed radioactively labeled chondroitin sulfate to rats and dogs and reported that more than 70% of that radioactivity was absorbed. That’s a huge difference when compared to what the Adebowale’s group reported. Why and how did that happen?
The answer isn’t that one study was wrong; it’s that the two groups measured different things. Adebowale tracked intact chondroitin disaccharides showing up in the blood, while Conte tracked a radioactive label that stays “stuck” to the molecule even after the gut chops the big chondroitin chain into fragments. The label counts all those fragments as “absorbed,” so it captures a much bigger number, even though a good chunk of that 70% is chondroitin bits and not intact chondroitin. The takeaway here is that bioavailability doesn’t mean much until you know exactly how it was measured.
Conte’s study did one more thing: it analyzed where the compound actually went. After oral dosing, the radioactive label didn’t just turn up in blood and urine but actually accumulated in synovial fluid and cartilage That’s pretty good evidence that orally dosed chondroitin (or at least its fragments) can reach target tissue. Although radioactive label itself isn’t proof that whole, working chondroitin arrived in useful amounts, it does show that the compound left the bloodstream and reached the joint.
Does supplement formulation matter?
Adebowale’s study is foundational, but it’s just one study- and it’s over 20 years old. I dug into the more recent literature and located a 2016 paper published by a team led by Lara Maxwell at Oklahoma State University. This study compared how well glucosamine was absorbed via 3 different formulations (liquid, chewable, tablet) in a randomized crossover design, with each dog serving as its own control across an 8-day dosing period.
This was the gist of the Maxwell et al. study:
Maxwell et al. (2016) Study Protocol
| Parameter | Details |
| Study Population | 8 dogs total |
| Products Tested | Glucosamine HCl or SO₃ in 3 formulations: liquid, chewable, tablet |
| Study Design | Randomized crossover; dogs as own controls |
| Group 1 (n=4) | Liquid + Tablet A |
| Group 2 (n=4) | Liquid + Tablet B |
| Dosing Protocol | Once daily for 8 days per formulation |
| Washout Period | 1 week between treatments |
| Key Variable | Formulation effect on absorption |
This study matters for two reasons. First, it’s not funded by a commercial supplement manufacturer. Second, it provides info a on whether the form of the supplement is a factor in how much is absorbed.
When the Maxwell team researchers accounted for the actual amount of glucosamine each product delivered, the overall extent of absorption was roughly similar across all three forms. However, the liquid form produced a noticeably higher peak plasma concentration (5.5 μg/mL) than the two tablets (3.1 and 2.1 μg/mL). It also got there far faster: the liquid hit its peak in about 0.7 hours, versus roughly 4 to 5 hours for the two tablets. So, the formulations delivered similar total amounts of glucosamine into the bloodstream, but the liquid form spiked higher and sooner.
Whether a higher, faster peak or a lower, steadier level matters more for an arthritic joint is not something this study can tell us. But what does matter here is the agreement across two independent studies, a Nutramax-funded one and a manufacturer-free one, a decade apart: oral glucosamine is absorbed in dogs, in real (though modest) amounts. The label dose still isn’t the absorbed dose — but the absorbed dose is not zero, and the way a product is formulated changes the shape of the curve.
Regarding the Adebowale study, a few other points are worth considering:
- The subjects were healthy youngish beagles, not senior or arthritic dogs. Gut absorption, hepatic metabolism, and joint tissue characteristics could differ in older dogs, or older dogs with conditions like osteoarthritis. (This applies equally to Maxwell’s dogs and Conte’s animals).
- The study reported plasma concentrations of the compounds and not what was in the actual joint tissue. When looking at arthritis, it’s only what reaches the cartilage that actually makes a difference. Blood-to-joint distribution is a separate step that this study did not measure. (Conte’s radiolabel study, discussed above, is the partial exception because it did detect label in synovial fluid and cartilage, though as fragments).
- The sample size (8 beagles) was small, and they were all the same sex, so it’s hard to say if what happens in a male beagle will also happen in an 80 lb. Husky. (Maxwell’s study was the same modest size, using eight dogs).
- Only one commercial product (Cosamin/Cosequin) and one formulation was studied. Maxwell broadened this slightly by testing three formulations.
- The study was funded by Nutramax Laboratories, the makers of the tested product. While it doesn’t necessarily mean the research was biased, it doesn’t entirely mean it’s a disinterested third-party here publishing this study. Having said that, the methodology appears rigorous, and a company willing to publish a 12% bioavailability number (hardly a slam-dunk marketing message) does suggest the research was honest.
7. What else can increase bioavailability
If 12% is the baseline for oral glucosamine HCl in beagles, the next question is, what could push that number higher?
The molecular form. The Adebowale study used glucosamine HCl. Glucosamine sulfate, the form more common in human supplements, has been studied more in human pharmacokinetics, naturally. Some human research suggests sulfate may have slightly better absorption characteristics, possibly because the sulfate ion actually plays a role in cartilage matrix synthesis. However, canine data comparing the two forms head-to-head are limited. The differences, where they exist, appear modest rather than dramatic.
The formulation. As the Maxwell data show, the same glucosamine dose delivered as a liquid versus a tablet produced a very different absorption curve. Form may not change how much gets in overall, but it changes how quickly and how high the compound spikes, which is at least worth knowing when a product markets itself as having “fast absorption.”
Co-administration with chondroitin. The Adebowale finding of 200-278% bioavailability for chondroitin with multi-dosing is striking. It suggests that combination products (which dominate the market) may be more meaningful than single-ingredient products, at least for chondroitin. Whether the actual combination has synergistic effects is debatable. Some in vitro studies suggest glucosamine and chondroitin together affect cartilage cells in ways neither does alone, but whether that can be viewed as synergistic is unclear.
Dosing frequency may matter more than total daily dose. Smaller doses given multiple times per day may achieve more consistent plasma concentrations than a single large daily dose. The Adebowale data on chondroitin accumulation do suggest this, especially regarding chondroitin.
Factors That May Increase Bioavailability
| Factor | Effect on Bioavailability | Evidence Level |
| Molecular Form | Glucosamine sulfate may have slightly better absorption than HCl | Modest; limited canine data |
| Formulation Type | Liquid formulations produce higher, faster peaks than tablets | Strong; Maxwell et al. 2016 |
| Combination Products | Chondroitin shows 200-278% bioavailability with multi-dosing | Strong; Adebowale et al. 2002 |
| Dosing Frequency | Multiple smaller doses may maintain steadier plasma levels | Moderate; suggested by accumulation data |
Note: Higher bioavailability does not automatically translate to better efficacy.
8. What this means in practice
What does 12% bioavailability mean for a senior dog?
It means meaningful but modest amounts of glucosamine reach circulation when the older dog takes supplements orally. The molecule isn’t trapped or discarded. It crosses the gut, survives the liver, and enters the bloodstream, where from it can theoretically reach its target tissue.
It certainly doesn’t mean supplements are worthless. Even modest plasma concentrations of a compound that’s a precursor for cartilage could, in principle, support joint health. The clinical trial evidence on whether this occurs is discussed in Part 2 of this series, and it’s more complicated than either supplement marketers will admit. Quite honestly, bioavailability alone is not enough to answer the efficacy question.
If you’re thinking about giving supplements to your dog, here are a few practical considerations from the research:
- The dose actually used in the published research is 1,500 to 3,000 mg of glucosamine per day for medium dogs. Products that contain less than this amount may not be delivering doses comparable to what’s reported.
- The form most studied in dogs is glucosamine HCl, not sulfate.
- Formulation affects the absorption curve. Per the Maxwell data, liquids tend to spike higher and faster than tablets, even when the total amount absorbed is similar. So “absorbs faster” marketing isn’t necessarily false — it’s just incomplete, since faster and higher isn’t the same as more.
- Combination products with chondroitin appear to be better due to chondroitin’s accumulation behavior.
- Premium “enhanced absorption” products charging significant markups should come with published data; if they don’t, the premium price isn’t backed by evidence.
- Consistency matters more than perfection. A supplement that’s actually given every day at a reasonable dose is more likely to benefit the dog than an optimal product that’s forgotten about.
9. Going to Part 2: Teaser
Bioavailability is the first question. The second is whether bioavailable glucosamine, once it reaches the bloodstream, actually helps arthritic joints. The clinical trial evidence on that question is genuinely mixed.
The studies that compare glucosamine-chondroitin to NSAIDs like carprofen tend to show that the supplement works, just less and more slowly than the NSAID. The studies that compare it to placebo show a much smaller and often insignificant effect. In fact, a 2017 review by Bhathal and colleagues (explored further in Part 2) surveyed this whole body of canine research, and their conclusion was sobering: while the tested products were safe, their actual clinical benefit remained uncertain, and largely because the available studies were so hard to compare. There were different manufacturers, salt forms, doses, durations, ingredient combinations, etc. and few well-designed trials among them.
Also, in Part 2 of this series, I’ll work through the McCarthy, Moreau, and Aragon papers, and explain why placebo-controlled and active-controlled trials produce different conclusions about the same supplement. Then, I’ll summarize what the data support. That summary will hopefully be more useful to you than the conclusions of supplement manufacturers.
The bottom line on bioavailability is, yes, glucosamine reaches the bloodstream when given orally. The dose that reaches circulation is meaningful but considerably less than the label dose implies. If that amount is enough to help an arthritic dog is the next question, and that’s the one Part 2 takes on.
Cited sources:
Adebowale A, Du J, Liang Z, Leslie JL, Eddington ND. The bioavailability and pharmacokinetics of glucosamine hydrochloride and low molecular weight chondroitin sulfate after single and multiple doses to beagle dogs. Biopharmaceutics & Drug Disposition. 2002;23(6):217–225.
American Pet Products Association (APPA), 2025 Dog & Cat Report: Key Trends in Pet Ownership.
Conte A, Volpi N, Palmieri L, Bahous I, Ronca G. Biochemical and pharmacokinetic aspects of oral treatment with chondroitin sulfate. Arzneimittelforschung. 1995;45(8):918–925. PMID: 7575762.
Dog Joint Supplements Market Size, Share, and Industry Trends Forecast 2026-2036 | MarkWide Research
Fact.MR Market Research Company. Dog Joint Supplements Market | Global Market Analysis Report – 2035
Maxwell LK, Regier P, Achanta S. “Comparison of Glucosamine Absorption After Administration of Oral Liquid, Chewable, and Tablet Formulations to Dogs.” J Am Anim Hosp Assoc 2016;52(2):90–94.
Hi, this is a comment.
To get started with moderating, editing, and deleting comments, please visit the Comments screen in the dashboard.
Commenter avatars come from Gravatar.